Critical Care in India is a booming specialty, especially in tertiary care hospital.With new technologies being introduced, the field is promising new dimensions andopportunities to help the patientsBy Ekta Srivastava, ENN
Critical Care in India is a booming specialty, especially in tertiary care hospital.With new technologies being introduced, the field is promising new dimensions andopportunities to help the patientsBy Ekta Srivastava, ENN
Ram Ashish, 22 years, male, suffering from Hypoxic Ischemic Encephalopathy (HIE), a condition that occurs when the entire brain is deprived of an adequate oxygen supply but the deprivation isnt total. He was unresponsive, BP was not recordable, there was no pulse and Cardiac monitor showed Ventricular Tachycardia (irregular heart activity in which heart cannot pump the blood). Immediately we incubated him, gave ventilator support, DC shocks were started. Then his Cardiac rhythm reverted to normal and all other drug supports started, says Doctor, Emergency, who saw him first.
While fixing the fault he climbed to the pole and accidently touched a high-tensioned wire. His co-workers immediately rushed him to the private hospital in Gurgaon. After his heart rhythm comes into normal condition he was shifted to Coronary Care Unit (CCU).Gradually all the drugs support and ventilator support under the supervision of cardio team, critical care team and neuron team was wined off and he was shifted to High Dependency Unit (HDU), which is a step down to ICU with a plan of discharge. This is the miracle of the Critical Care and its experts, which can bring the hopes back to people who are about to lose their loved ones.

Critical Care offers intensive care towards patients who are very sick. Life threatening illness which requires intensive monitoring that cannot be provided in general wards andyet to be monitored continuously are put under ICU. There are specific types of CCUs that cater to a particular category of patients, for e.g., CCUs that admit patients suffering from a heart attack, cardio-thoracic or neurosurgical, ICU that admit cardiac or neurosurgical patients, burns ICU that admit patients with burns, neo-natal ICU that admits newborns, PICU or pediatric ICU that admits children with critical illness etc. This is a generic term applied to a specialised area/unit of a hospital (usually a tertiary care hospital) equipped and staffed to provide life- sustaining therapy to critically ill patients with reversible pathology. So, Critical Care is basically Intensive Care which is done by a team of doctors and other supporting staffs.
Technologies
Equipments like monitors, intravenous(IV) tubes, feeding tubes, catheters,breathing machines, and other equipmentare common in critical care units.While speaking about the Indian scenarioDr Abhay Patwari, FarwaniyaHospital, says that, most of the equipmentis imported. Some small companies are coming up with manufacturing equipment. Most used machines like ventilation machines, dialysis machines, echo machines are to be imported from outside India. It will be really helpful if some companies come forward along with collaboration with some big hospitals. We are ready to accept them if the quality is good. However, when there are almost every International standard facilities are being given in tertiary care hospitals most of the community based and secondary hospitals are lacking from the forefront.
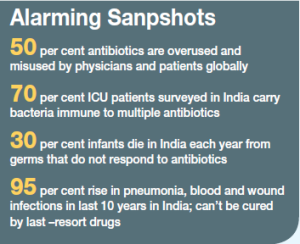
Excessive use ofanti-biotics in Critical Care
If you want to use Penicillin, use it in right dose
Sir Alexander Fleming
Anti-biotic, one millionth of a milli-meter in size, these invisible malevolent bacteria has challenged the whole medical and scientific fraternity against their development and progress about these miracle drugs. Experts believe that a hidden epidemic is upon us. According to them the reason they depict is doctors prescribing longer courses of antibiotics and the antibiotics becoming more expensive, which shows that anti-biotic resistance(ABR) is rising. For a long time there has been a talk of unjustified and excessive use of antibiotics in the critical care, when Dr Abhay Patwari, Farwaniya Hospital said, Antibiotic resistance in the ICU is a huge problem and unwise use over the next few years will leave us vulnerable to infection by resistant organisms. A prudent antibiotic policy must be developed and therapy should be tailored to the narrowest spectrum possible. Lot of emphasis and training must go to preventinfection rather than treat it. The assistance of a clinical microbiologist is a must to guide antibiotic therapy.
Now , here are not just todays experts who are giving caution about the excessive and unjustified use of antibiotic but the smart guy of evolution Alexander Fleming also cautioned on the day he received the Nobel Prize for discovering penicillin in 1945 that antibiotics would lead to a bacterial backlash.
From where drugs become bugs
Unfortunately, antibiotics in India are Over the Counter drugs (OTC) drugs and most of the higher antibiotics are available without the prescription. That is the reason the use are more in clinics and smaller hospitals and by the patients who get the names of the antibiotics from the Google and then shall procure it from the chemist shop.
In most of the hospitals Critical Care heads believes that most of the time when patients come to the tertiary care centre they were already loaded with higher antibiotics. As Dr Omender Singh, Max Healthcare said, Most of the time when patients arrive in the hospital they already have all the antibiotics because they are easily accessible, you go to any chemist they will give you that and then we cant try the same antibiotics because the bugs get resistance. That is when they landed up with the resistance bugs in the hospitals then we have to use higher antibiotics. On similar situation further adds Dr Yatin Mehta, Medanta, The Medicity, Now these higher antibiotics , they can cause up to ` 10,000 for oneday therapy, and say if you are giving it for 10 days then the bill cost will be like `100,000 plus your antibiotics organism are also growing up. The million dollar question here is from where are they getting to becomes anti-biotic resistance ( ABR) and so said Dr Mehta, Chairman Critical Care Every homeopathic doctor is prescribing the antibiotics, chemist are giving that .Why should be they allowed to do so? He is not a doctor. So, its start from there. Then the General Practitioner (GP) they do the same and then there are doctors in the tertiary care also who are mis-handling the antibiotics
 Indian doctors casual way
Indian doctors casual way
In a survey made by WHO in 2005 reports that antibiotic consumption in India has gone up to seven percent annually, while reports also reveals that 53 per cent of Delhi ites self prescribe antibiotics; one in four skips the course once they feel better; and 18 per cent physicians prescribe antibiotics for common cold. Also, very powerful drugs, meant for hospital use, were being routinely dispensed, even for common infections. Even the scenario dose not endshere as experts said Indian doctors are very much casual about using antibiotics even in children, say if a patient is doing well then they dont want to change the medicine and let it to be continued. Now we are seeing multi-drug resistance organism which were initially only in hospital environment are now present in the community.
While it is believed that doctors must be aware of the havoc caused by these anti-biotic the first question that arise is why still they are prescribing them in such a huge manner, as Dr Mehta Says, In the bigger sectors, yes they knew but in other pe-ripheries they are not aware of this. So we need to penetrate the peripheries more with the knowledge, hazards of misuse of antibiotics and we have to tell them to avoid it
Governments Plan of action
Recently, Health and Family welfare Minister Ghulam Nabi Azad during the Budget session of Parliament faced the fierce questioning on the rising tide of ABR and an urgent question hang over the future: What if antibiotics do not work anymore? Even the WHO during the 2013 World Economic Forum (WEF) in Davos, where WEF consider this as the one of the chief threats to human health for which the world is mostly unprepared to cope with. Off course Government is talking about it but they should put some restriction as who should prescribe it or only hospital doctors can prescribe such higher antibiotics instead of local GP MCI and IMA, they should play more active role said, Dr Mehta. Same way Dr Singh, believes that government is taking a step forward like most of the antibiotics and some of the drugs need doctors prescription actually while he insist on the fact that all the antibiotic should required a prescription from the physician . India needs an antibiotic policy and a national registry, inclusion of ABR in medical courses, monitoring of pharmacies so that antibiotics cannot be sold without prescription and ensuring infection-control protocols in hospitals. We are in a dangerous zone where life can end in any unexpected way, there is no antibiotic in the pipeline in the next 10 years. So we are finished if we dont deal with this at this level. Stop the misuse of antibiotics said Dr Mehta.
End note
In order to understand more aboutCritical Care we talk to heads of CriticalCare divisions of major hospital.
 Like
Like
 Dislike
Dislike
Be a part of Elets Collaborative Initiatives. Join Us for Upcoming Events and explore business opportunities. Like us on Facebook , connect with us on LinkedIn and follow us on Twitter , Instagram.