Research
10.81% decline in People with Desirable Cholesterol Levels: Metropolis Healthcares Analysis
10.81% decline in People with Desirable Cholesterol Levels: Metropolis Healthcares Analysis
![]() By eHealth Network - 29 September 2016
By eHealth Network - 29 September 2016





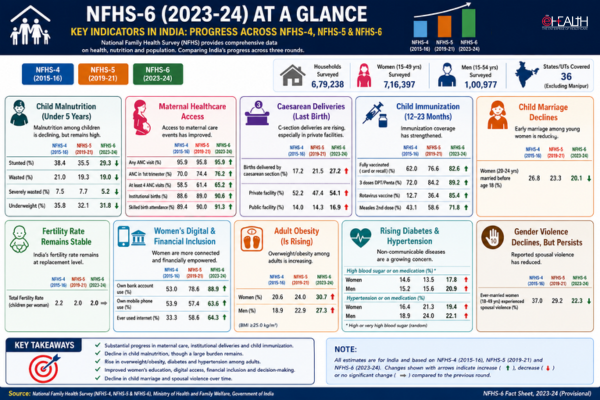
According to a recent study by Metropolis Healthcare Ltd., over 50 percent of 40,000 samples tested for cholesterol showed borderline high, high or very high levels of Non-HDL levels. 57.42 percent of samples tested between Borderline High to Very High for non-HDL levels, up from 46.62 percent in 2011.
Data reveals that total cholesterol in the year 2011 was within desirable levels for 72.86% of the samples, borderline high for 20.36% of the population and high for 6.87% of the population. For the year 2015, 67.77% of the population was within desirable levels, 22.88% of the population was borderline high and 9.35% of the sample population was high.
Similarly for Non HDL 53.39% of the population reflected desirable levels, 25.26% borderline high, 14.03% high and 7.33% very high for the year 2011. However, for the year 2015, 42.58 % of the population had desirable levels of Non HDL cholesterol, while 27.61% of the population had borderline high levels, 17.89% had high levels and 11.92% had very high levels. Overall data has revealed that there is a clear five percent shift to dyslipidaemia from desirable levels.

Dr. Puneet K Nigam, Senior Vice President from Metropolis Healthcare said, A growing body of evidence indicates that atherosclerosis begins early in life. Furthermore, studies show that the presence and severity of atherosclerotic lesions in children and young & elderly adults are related to serum lipid levels. American Academy of Paediatrics, American Heart Association, and NCEP guidelines recommend – Children older than 2 years who have CAD risk factors or a family history of CAD or dyslipidaemia, and children for whom family history is not known, should be screened for dyslipidaemia; these patients should be rescreened every 3 to 5 years; if lipid levels are within acceptable ranges. In all adolescents older than 16 years, screening should be repeated every 5 years or more frequently for patients with CAD risk factors or a family history of CAD. All Middle-aged adults & older adults should be screened annually.

| Parameter | Year | Desirable | Borderline High | High | Very High |
| Total Cholesterol | 2011 | 72.86 % | 20.36 % | 6.78 % | NA |
| Total Cholesterol | 2015 | 67.77 % | 22.88 % | 9.35 % | NA |
| Non HDL | 2011 | 53.39 % | 25.26 % | 14.03 % | 7.33 % |
| Non HDL | 2015 | 42.58 % | 27.61 % | 17.89 % | 11.92 % |
* 8% calculated based on difference in Non HDL levels among the High and Very High segments
There are various risk factors which contribute to dyslipidaemia – Family history of CAD, Familial Hypertriglyceridemia, Hypertension , Dietary Risk Factors: Fats, Diabetes, Obesity and Overweight, sedentary life styles, and Cigarette smoking . He continued Bringing down non-HDL-C dependably starts with migrating to healthy lifestyle; generally, one should cut out calories, Trans unsaturated fats and exercise regularly. In any case, lessening sugar intake is exceptionally important for bringing down levels of triglycerides and non-HDL-C, especially in over weight individuals.
Nourishments that are high in omega-3 unsaturated fats may likewise be valuable for reducing non-HDL Cholesterol. Fish like salmon, sardines, mackerel, and herring is rich in omega-3 which is an extremely sensible option.
Periodic Testing “ Lipid Profile along with relevant investigations are recommended. Testing every 5 years is recommended for the ages 45 “ 75, Every 12 months if one is on cholesterol lowering medication, any child of a parent with inherited high cholesterol by the age of 10 and first degree relatives of a person with high cholesterol on being told of the risk.
Cholesterol is a fat-like substance (lipid) that is present in cell membranes and is a precursor of bile acids and steroid hormones. Normally cholesterol travels in the blood in distinct particles containing both lipid and proteins (lipoproteins). In modern times, non-HDL cholesterol (non-HDL-C) has become a commonly used marker for a blood lipid pattern associated with increased risk of heart disease.
Atherosclerosis is the most well-known and the fundamental reason for cardiovascular diseases. Atherosclerosis is a condition where the arteries become narrowed and hardened due to an excessive build-up of plaque in the artery wall, which is formed by accumulation of Non HDL Cholesterol, which leads to CAD. It is generally mediated by a complex interaction between lipoproteins, white blood cells and the normal components of the arterial wall. It is also to be considered that Lipoproteins are the particles that vehicle cholesterol and triglycerides in the blood circulation system. These Lipoproteins that are actively involved in atherosclerosis are better known as atherogenic and predominantly carry cholesterol and other types of fats such as triglycerides. The three major components that are measured and tested in abasic lipid profile are total cholesterol, triglycerides, and HDL-C.
Non-HDL-C on the other hand has been shown to be a better marker of risk in both primary and secondary prevention studies. According to the results of a recent analysis of data combined from sixty eight studies, non-HDL-C turned out to be the best risk predictor of all cholesterol measures, both for CAD (Coronary Artery Disease) and for strokes.
Dyslipidemia is a primary and major risk factor for CAD and may even be a prerequisite for CAD, occurring before other major risk factors come into play. Epidemiologic data also suggest that hypercholesterolemia and perhaps coronary atherosclerosis itself are risk factors for ischemic stroke.
Medical professionals typically test cholesterol levels through medical check-ups and in order to uate blood cholesterol, blood test known as a lipid panel, as well as lipid profile is conducted.

 Like
Like
 Dislike
Dislike
Be a part of Elets Collaborative Initiatives. Join Us for Upcoming Events and explore business opportunities. Like us on Facebook , connect with us on LinkedIn and follow us on Twitter , Instagram.
"Exciting news! Elets technomedia is now on WhatsApp Channels Subscribe today by clicking the link and stay updated with the latest insights!" Click here!